

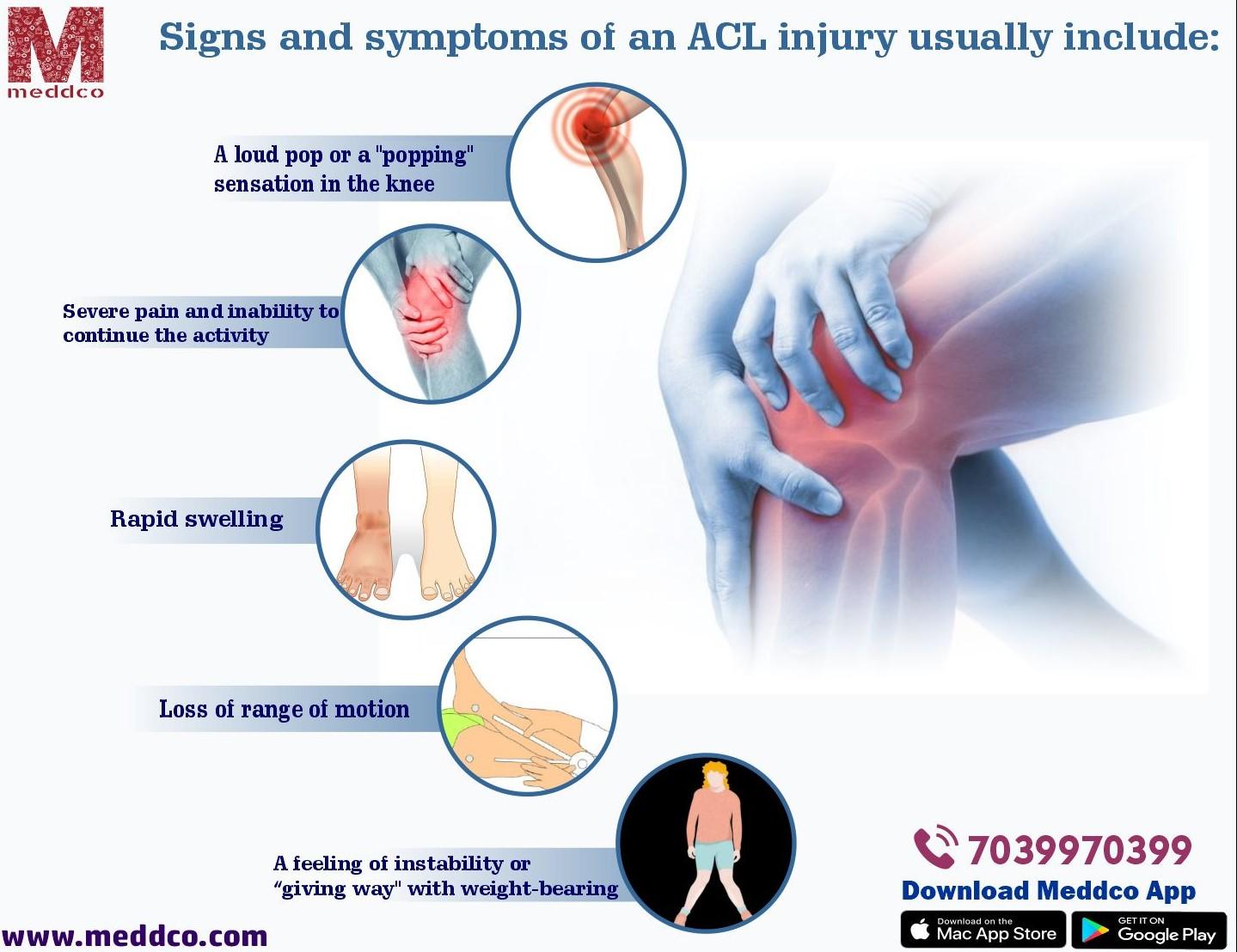
The Anterior Cruciate Ligament is the ligament that stabilizes the knee. Anterior Cruciate Ligament injury is a common occurrence, particularly among sportspeople. Anterior Cruciate Ligament (ACL) reconstruction is a popular procedure. Based on the type of injury, ACL injuries can be divided into contact and non-contact. A contact injury occurs when a person or item collides with the knee, tearing the ligament. Non-contact tears, on the other hand, are most common when decelerating, cutting, or landing from a jump. Females are 4-6 times more likely than males to sustain ACL damage. In high school, ACL injuries account for one-quarter of all knee injuries.
The femur (thighbone) meets the tibia (shin bone) at the knee, a hinge joint. These four ligaments, which attach bones, keep this vital joint together:
an anterior cruciate ligament (ACL)
medial collateral ligament (MCL),
lateral collateral ligament (LCL)
cruciate ligament, posterior (PCL).
The ACL runs diagonally between the femur and the tibia, preventing the tibia from slipping forward. It also gives the knee stability when it rotates from side to side.
What is ACL Reconstruction?
During ACL surgery, the anterior cruciate ligament is repaired or rebuilt (ACL). The ACL is a major soft-tissue component of the knee that connects the femur to the tibia. ACL tears, whether partial or complete, are prevalent among athletes. ACL reconstruction surgery, in which the torn ligament is replaced with a tissue graft to imitate the standard ACL, is commonly performed by sports medicine experts and orthopedic surgeons. HSS, on the other hand, takes a multidisciplinary approach to treating ACL injuries, collaborating with physiatrists, sports medicine physicians, orthopedic surgeons, and imaging and rehabilitation specialists to establish the best treatment option for each patient. People who have had an ACL injury are more likely than those who have not developed osteoarthritis in the knee early in life. HSS clinicians and scientists are constantly researching ACL surgery approaches to better patients' short- and long-term outcomes.
The reason behind Reason
The need for surgery is determined by the degree of the ACL injury and the patient's lifestyle. An ACL that has been torn will not mend on its own. However, studies have shown that in some people with a partial tear of the ACL, the ligament can recover without surgery.
One of the most frequent knee injuries is an ACL tear, especially common among persons who participate in high-impact sports like basketball.
- football
- soccer
- skiing
- hockey
According to the American Academy of Orthopaedic Surgeons, most of these injuries occur without the involvement of another player (AAOS). They usually happen when a player twists or pivots during a game.
Necessary tests for ACL Reconstruction
A doctor will undertake two manual exams to identify whether a tear is partial or complete:
Lachman test: The doctor will attempt to separate the shin and thigh bones. The bones will not move just slightly if the ACL is ruptured but still intact.
Pivot Sheet Test: The patient lies on their back as the doctor elevates their leg and applies rotating pressure to the knee. The test is negative if the bones do not shift.
It may recommend postponing surgery in patients with a partial tear and waiting to see if the ligament heals without it.
How soon should you get ACL surgery?
Reconstruction surgery for a total ACL tear is usually scheduled between three and six weeks after the injury occurs. It reduces inflammation in the affected area. Patients who have surgery too early may develop arthrofibrosis, a severe scarring response.
Orthopedic doctors decide whether to perform reconstruction surgery based on the following factors: • whether any other ailments need to be treated first
- the knee's physical appearance
- the severity of the patient's suffering
- the patient's range of motion and muscle control when bending (bending) or straightening (straightening) their leg.
According to some research, I am delaying ACL reconstruction surgery for six months or more after damage diminishes the likelihood of a clinically significant outcome and increases the possibility of future revision surgeries.
Risks of ACL Reconstruction
Any anesthetic carries the following risks:
- Allergies to medications
- Breathing difficulties
Any procedure carries the following risks:
- Bleedings
- Infection
Other hazards associated with this operation include:
- A blood clot in the leg
- The ligament failing to repair
- The surgery failed to improve symptoms
- An injury to a neighboring blood vessel
- Knee pain
- Knee stiffness or loss of range of motion
- Knee weakness
Surgical Choices
Autograft of knee tendons.
The patellar tendon autograft uses the patient's middle third of the knee-tendon and a bone plug from the shin and kneecap. It is frequently advised for high-demand sportsmen and patients whose jobs do not involve a substantial amount of kneeling, some surgeons as the "gold standard" for ACL restoration.
The graft failure rate was lower in the patellar tendon group in studies comparing the outcomes of the patellar tendon and hamstring autograft ACL restoration. Furthermore, when this graft is compared to others, most studies indicate equivalent or better results in postoperative tests for knee laxity (Lachman's, anterior drawer, and instrumented tests).
However, postoperative patellofemoral discomfort (pain behind the kneecap) and associated complications are more common with patellar tendon autografts.
The following are the drawbacks of a patellar tendon autograft:
1. Pain behind the kneecap after surgery
2. Pain when kneeling
3. Slightly higher risk of postoperative stiffness
4. Low chance of patella fracture
Autograft of hamstring tendon
The hamstring tendon autograft for ACL restoration is made from the semitendinosus hamstring tendon on the inner side of the knee. The gracilis tendon, attached below the knee in the same location, is used by certain surgeons. A two- or four-strand tendon transplant is the result. Proponents of the hamstring graft argue that harvesting the graft is easier than gathering the patellar tendon autograft, claiming that:
- Fewer problems with anterior knee discomfort or kneecap pain after surgery
- Fewer problems with postoperative stiffness
- Smaller incision
- Quicker recovery
As the transplant does not have bone plugs, the strength and kind of fixation in the bone tunnels may limit the graft's effectiveness. Whether hamstring grafts are slightly more vulnerable to graft extension (stretching), which may lead to higher laxity during objective testing, has been debated in research investigations. Some studies have recently shown that patients' hamstring strength decreases after surgery. Patients with intrinsic ligamentous laxity and knee hyperextension of 10 degrees or more may have a higher risk of postoperative hamstring graft laxity on clinical examination. As a result, some doctors advise using patellar tendon autografts in hypermobile individuals.
Furthermore, because the medial hamstrings frequently provide dynamic support against valgus stress and instability, some surgeons believe that chronic or residual medial collateral ligament laxity (grade 2 or more) at the time of ACL reconstruction may be a contraindication for using the patient's semitendinosus and gracilis tendons as an ACL graft.
Autograft of the knee joint Patients who have already had their ACL repair fail are frequently given a quadriceps tendon autograft. A bone plug is used from the higher end of the knee cap and the middle third of the patient's quadriceps tendon. For taller and heavier patients, this results in a larger graft. The fixation is not as strong as the patellar tendon transplant since only a bone plug is on one side. Postoperative anterior knee discomfort is highly associated with a low chance of patella fracture. Patients may find the incision unattractive from a cosmetic standpoint.
Allografts
Allografts are cadaveric grafts that are becoming increasingly common. These grafts are also used to heal or reconstruct multiple knee ligaments in patients who have had previous ACL reconstructions fail. The use of allograft tissue has several advantages, including reducing discomfort associated with obtaining the graft from the patient, reduced surgical time, and smaller incisions. The patellar tendon allograft enables secure bony fixation with screws in the tibial and femoral bone tunnels.
Despite meticulous screening and processing, allografts are associated with a risk of infection, including viral transmission (HIV and Hepatitis C). Improvements in transplant tissue testing and processing processes have resulted from several deaths attributed to bacterial infection from allograft tissue (due to faulty procurement and sterilization techniques). There have also been mixed results in investigations on whether allografts are slightly more prone to graft elongation (stretching), leading to higher laxity during testing.
Some published research suggests that using allografts for ACL reconstruction leads to a higher failure rate. Allografts had a higher failure risk in young, active patients returning to high-demand sporting activities following ACL surgery compared to autografts.
It's unknown why this increased failure rate exists. It could be attributable to the qualities of the graft material (sterilization processes used, graft donor age, storage of the graft). The athlete's ill-advised early return to the sport could result from a perceived faster physiologic recovery. The graft is not biologically ready to be loaded and strained during athletic activity.
How you prepare
Physical treatment will most likely be required before your operation. Reduce discomfort and swelling before surgery, restore complete range of motion in your knee, and strengthen muscles. People who have a stiff, swollen knee before surgery may not be able to regain a complete range of activity afterward.
As an outpatient treatment, ACL restoration allows you to return home the same day. Make arrangements for a ride home.
Food and medications
Any drugs or dietary supplements you take should be disclosed to your surgeon. If you take blood-thinning medications regularly, your doctor may advise you to stop taking them for at least a week before surgery to lessen the chance of bleeding.
The night before your operation, follow your doctor's instructions on stopping eating, drinking, and taking any other medications.
What you can expect
ACL reconstruction is usually done under general anaesthesia, so you'll be asleep for the procedure. Small incisions are used to hold a thin, tube-like video camera and provide surgical instruments access to the joint space during ACL restoration.
During the procedure
Your injured ligament will be removed and replaced with a tendon segment by your surgeon. A graft is a piece of replacement tissue from another part of your knee or a tendon from a deceased donor.
To correctly position the graft, your surgeon will drill sockets or tunnels into your thighbone and shinbone, which will be fastened to your bones with screws or other devices. The graft will act as a framework for the growth of new ligament tissue.
After the procedure
You can go home the same day after you recover from anesthesia. You'll practice walking with crutches before returning home, and your surgeon may ask you to wear a knee brace or splint to safeguard the graft.
After surgery, your doctor will give you precise advice on managing swelling and pain. Keep your leg elevated as much as possible, put a cold wrap or ice on your knee, and rest as much as possible.
Over-the-counter medications like acetaminophen (Tylenol), ibuprofen (Advil, Motrin IB, and others), or naproxen sodium can aid with pain relief (Aleve). More potent pain relievers, such as meloxicam (Mobic), tramadol (Ultram, Qdolo, ConZip), or oxycodone (Ultram, Qdolo, ConZip), may be prescribed by your (OxyContin, Roxicodone, others).
Follow your surgeon's instructions for how long to freeze your knee, how long to use crutches, and when it's safe to put weight on it. You'll also be instructed when to wash or bathe, when to change the wound dressings, and how to handle post-surgery care.
After ACL surgery, progressive physical therapy helps to strengthen the muscles around your knee and increase flexibility. A physical therapist will show you how to conduct exercises that you can do at home or with continuing supervision. It is critical to stick to the rehabilitation plan to heal correctly and achieve the best possible results.
Recovery Room
You'll spend at least two hours in the recovery room after ACL reconstruction surgery as the anesthetic wears off. They will wrap your knee and may apply an ice pack to relieve pain.
When you feel the pain coming on, ask for pain medicine. Pain medication is most effective when pain begins to emerge rather than when it has gotten severe. Pain medication will be
either orally or intravenously. A nurse will administer the dosage your doctor has ordered and believes to be safe.
While in the recovery room, move your feet to enhance circulation. Your surgeon may recommend utilizing crutches or a cane for two to three weeks. Within two weeks, the majority of patients can walk without crutches.
You might be allowed to go home after you're completely awake. Your nurse and doctor will decide whether you are ready to leave the hospital or if you will need to stay overnight.
If you don't already have one, you'll be offered a follow-up appointment and a prescription for pain medication before you leave. You will be sleepy and unable to drive, so make arrangements for transportation home before surgery.
Results of ACL Reconstruction
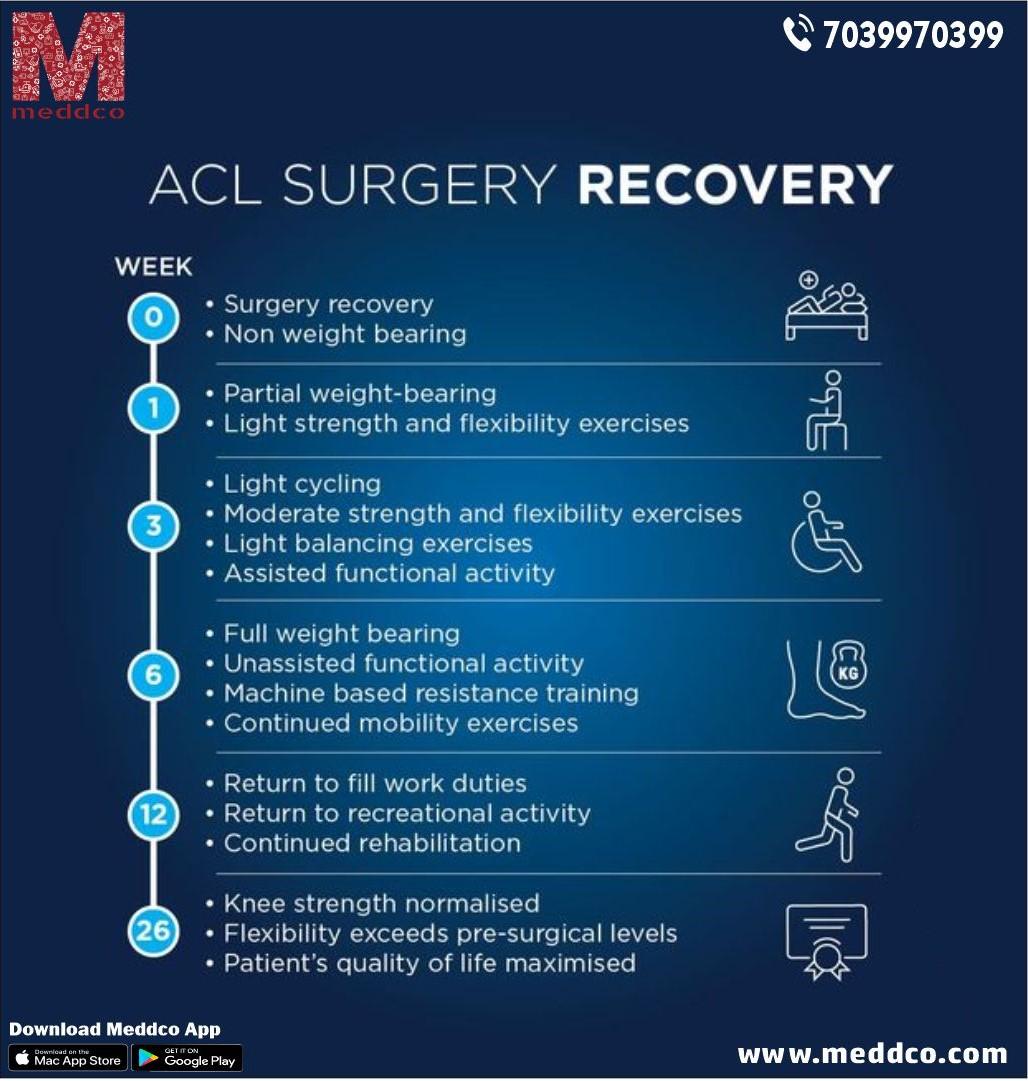
ACL repair combined with targeted therapy can usually restore knee stability and function. It would help if you tried to regain a range of motion similar to your opposite knee within the first few weeks after surgery. The average recovery time is nine months. Athletes may have to wait eight to twelve months to return to their sports.
MEDDCO.COM is India's first digital pricing online platform, where price transparency is the key. Our website allows user to search for surgical procedure diagnostic test and other healthcare services amongst various hospital and healthcare provider in and around the location of user to compare the cost of services, compare the quality of services by the user rating/reviews to take informed decision.
On our website you can find the best package price for ACL Reconstruction. You can also book an online appointment through our website.
For more information visit our website





